By Dr. Shyam D, MCh Neurosurgery | Apollo Hospitals, Madurai | Updated April 2026
If your doctor has recommended spine surgery, you don’t have to imagine a long scar, weeks in bed, or months away from work. Modern minimally invasive techniques have changed everything.
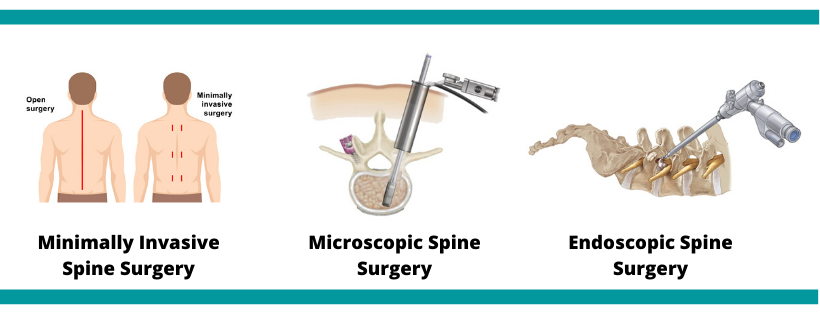
WHAT EXACTLY IS MINIMALLY INVASIVE SPINE SURGERY?
Minimally invasive spine surgery (MISS) is a collection of advanced surgical techniques that allow neurosurgeons to treat spine problems through very small incisions — sometimes as tiny as 1 centimetre — using specialised instruments, cameras, and real-time imaging guidance.
Unlike traditional “open” spine surgery, which requires cutting through large areas of muscle and tissue to reach the spine, MISS targets the problem precisely, leaving the surrounding healthy tissue almost completely intact.
“Think of it like keyhole surgery for your spine. We reach the exact problem — a slipped disc, a compressed nerve, an unstable vertebra — fix it, and come out, without disturbing anything that doesn’t need to be touched.” — Dr. Shyam D, Neurosurgeon, Apollo Hospitals, Madurai
WHY ARE PATIENTS IN MADURAI CHOOSING MISS?
Madurai is a city on the move. Whether you are a government employee commuting daily, a construction worker, a textile mill operator, a homemaker, or a farmer, back pain can take you away from your livelihood. The fear of surgery, long hospital stays, and slow recovery stops many people from getting the help they need.
Minimally invasive spine surgery directly addresses these fears.
Traditional Open Surgery:
- 10–15 cm incision
- Large muscle cutting and retraction
- 5–7 days hospital stay
- Significant post-operative pain
- 3–6 months recovery
- High blood loss, often needing transfusion
Minimally Invasive Surgery:
- 1–3 cm tiny incision
- Muscles gently moved, not cut
- 1–2 days hospital stay
- Minimal post-operative pain
- 2–6 weeks recovery
- Minimal blood loss, rarely needs transfusion
WHICH SPINE CONDITIONS CAN BE TREATED WITH MISS?
A common misconception is that minimally invasive surgery is only for simple or minor spine problems. In reality, experienced neurosurgeons can now treat a wide range of complex conditions using this approach:
- Lumbar disc herniation (slip disc)
- Cervical disc disease and neck pain
- Spinal stenosis (narrowing of the spinal canal)
- Degenerative disc disease
- Spondylolisthesis (slipped vertebra)
- Sciatica not responding to medicines
- Spinal tumours (selected cases)
- Spinal fractures and trauma
- Spinal infections and TB of the spine
- Craniovertebral junction disorders
Note: Not every spine condition is suitable for minimally invasive surgery. Your surgeon will evaluate your MRI, CT scan, and clinical condition to recommend the most appropriate approach for you.
HOW DOES THE SURGERY ACTUALLY WORK?
Understanding the process can ease a lot of anxiety. Here is what happens during a typical minimally invasive spine procedure:
- Anaesthesia: You are placed under general or spinal anaesthesia. You feel nothing throughout the procedure.
- Tiny incision: The surgeon makes one or two small cuts — often just 1 to 2 cm — at the target area of your spine.
- Tubular retractor placement: A series of progressively larger dilators are inserted to gently push aside the muscle, creating a working tunnel to the spine without cutting the muscle.
- Surgical microscope or endoscope: A high-definition camera or operating microscope gives the surgeon a magnified, illuminated view of the spine through this small tunnel.
- The repair: The surgeon removes the problematic disc material, decompresses the nerve, fuses vertebrae, or places screws and rods — depending on what is needed.
- Closure: The tiny incision is closed with absorbable sutures or surgical glue. No large wound to manage at home.
- Recovery: Most patients are walking within hours of surgery. Many go home the very next day.
COMMON MISS PROCEDURES PERFORMED IN MADURAI
Microdiscectomy The most common MISS procedure in Madurai. A tiny camera and microsurgical tools are used to remove the fragment of a herniated disc that is pressing on a nerve. Patients with sciatica and leg pain often experience immediate relief after this procedure.
Endoscopic Spine Surgery An endoscope (thin tube with a camera) is inserted through a small incision. The surgeon watches the procedure on a monitor and operates using instruments passed through the same tube. Excellent for disc herniations at multiple levels.
Minimally Invasive Lumbar Fusion (TLIF / PLIF) For patients with spondylolisthesis or severe instability, the vertebrae are fused together using screws, rods, and bone graft — all placed through tiny incisions using computer-guided navigation. This stabilises the spine permanently with far less trauma than open fusion.
Percutaneous Pedicle Screw Fixation Screws are inserted into the vertebrae through skin punctures without any open incision. Ideal for spinal fractures and trauma cases, especially after road accidents — a very common need in Madurai.
Vertebroplasty and Kyphoplasty For elderly patients with osteoporotic spine fractures, a special medical cement is injected into the collapsed vertebra through a needle. Pain relief is dramatic, often felt the same day.
WHO IS THE IDEAL CANDIDATE FOR MISS?
You may be a good candidate for minimally invasive spine surgery if you have any of the following:
- Persistent back or leg pain that has not improved with 6–12 weeks of physiotherapy, pain medication, or injections
- Weakness, numbness, or tingling in the arms or legs caused by nerve compression
- Difficulty walking, standing, or performing daily activities
- An MRI or CT scan showing a clear structural cause — a herniated disc, bone spur, or narrowed spinal canal
- A spine fracture, tumour, or infection requiring surgical treatment
Patients with uncontrolled diabetes, severe cardiac issues, or extremely complex multi-level disease may need additional evaluation to determine the safest approach.
RECOVERY — WHAT TO EXPECT WEEK BY WEEK
Day 1–2: Walking with support. Discharge from hospital. Mild soreness at the incision site.
Week 1–2: Light walking daily. Avoid bending and lifting. Wound heals well.
Week 3–4: Most patients return to desk work. Physiotherapy begins. Leg pain resolves significantly.
Week 6–8: Return to normal activities. Driving allowed. Manual workers begin graded return.
Post-operative pain is significantly less than with open surgery. Most patients manage well with oral pain medications for a few days. The nerve or back pain that brought you to surgery often starts improving quickly after the procedure.
ABOUT THE AUTHOR
Dr. Shyam D MCh Neurosurgery | International Fellow, American Association of Neurological Surgeons (IFAANS) | Fellow, American College of Surgeons (FACS) | Cerebrovascular Fellow, Japan | Advanced Skull Base Surgery, USA Consultant Neurosurgeon, Apollo Hospitals Madurai
📞 +91 63802 71088 📧 drshyamsbrainandspine@gmail.com 🌐 www.drshyam.com
Not sure if MISS is right for you? Share your MRI or CT report with Dr. Shyam for a personalised opinion. Consultations available in person at Apollo Hospitals Madurai and online via WhatsApp.
